Often discovered by chance during a colon cancer screening, diverticular disease is rather a widespread digestive disease, especially in countries like Australia, where we generally tend to eat a low-fibre diet.
What is diverticulitis?
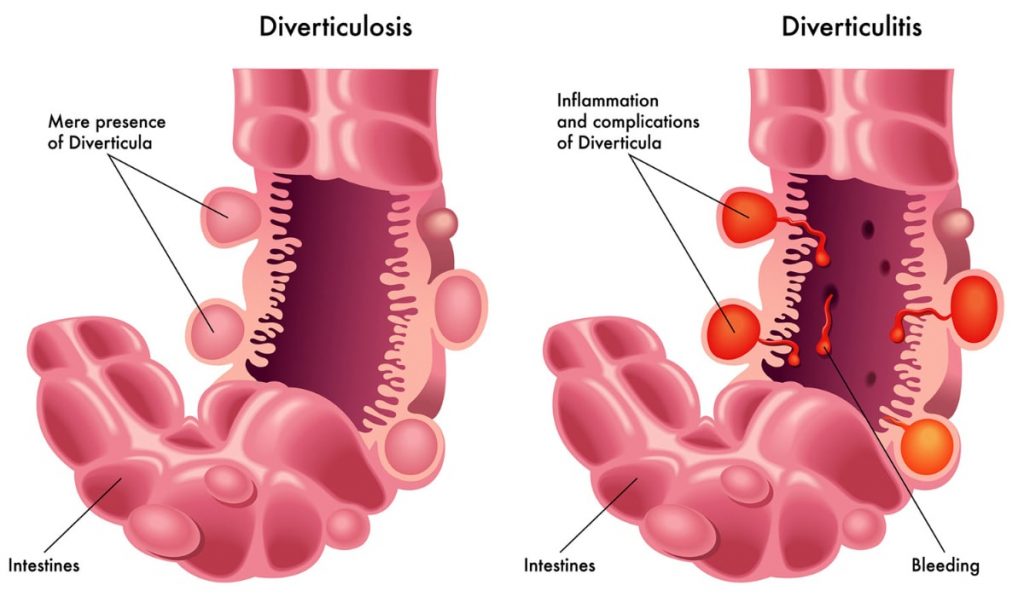
It starts as diverticulosis; the mere presence of small pouches or outpouchings in the lining of your intestine. These pouches remain harmless, but when they become infected and inflamed, it turns troublesome, causing a condition known as diverticulitis (Thompson, 2009).
And just like many other digestive diseases, diverticular disease is also characterised by symptoms such as changes in your bowel habits, bloating, diarrhoea, gas formation, and abdominal cramping.
At the same time, it is also possible that people would be completely unaware of their condition because diverticular disease can be asymptomatic too (MedicalNewsToday, 2018).
How is diverticular disease formed?
When healthy, the pouches formed are nothing to be worried about.
It often starts in the weakened areas of the colon. The lack of fibre in diet predisposes to constipation, requiring higher pressure to push out the stool and possibly causing the bowel’s lining to protrude outside.
And with recurring constipation, deposits of bacteria and faeces can form in the pouches, turning them inflamed and infected, potentially requiring immediate medical help from a specialist like a gastroenterologist.
What causes diverticular disease?
Age is a significant risk factor when discussing diverticular disease. It primarily affects older people, about 1 in 3 Australians aged over 45 have diverticular disease (Healthdirect Australia, 2018). A study has also confirmed that diverticular disease is rare before the age of 40 (Marinella and Muhanad, 2000).
Doctors believe that the lack of fibre in our diet is a factor that leads to diverticular disease. This is why diverticular disease is relatively uncommon in parts of the world that have a diet rich in fibre.
Research also suggests that environment and genetics may be responsible too. A study on familial diverticulitis indicates that genetics may account for 40% – 53% of disease incidence (Coble et al. 2017).
What are the complications of diverticulitis?

1) Abscess
The most common complication of diverticular disease is the presence of an abscess which is a pus-filled lump around the infected area. According to a study, up to 30% of patients develop abscesses when diagnosed with diverticulitis (Onur et al, 2016).
2) Bowel Obstruction
Bowel obstruction occurs when the inflammation is too intense to let pass stool due to bowel narrowing. This can be a medical emergency requiring surgery. However, a partial blockage can cause similar symptoms but does not necessarily require surgery.
3) Fistula
Fistula occurs when the infected tissue sticks together. It can lead to the bacteria in your large intestine travelling to other parts of your body, triggering infections, such as an infection of the bladder.
4) Peritonitis
Peritonitis is caused when an infected pouch splits, causing the bacteria to enter the abdominal cavity from the GI tract (NHS Inform, 2016). They often require immediate medical intervention through medicines and antibiotics or surgery to remove the pus if deemed necessary by a gastroenterologist.
Diagnosis and treatment of diverticular disease
Diverticular disease often occurs without any visible symptoms. And when symptoms appear, they resemble several other gastrointestinal conditions.
This is why diverticular disease tends to be diagnosed during screening for other diseases such as colon cancer (Betterhealth, 2012).
Several medical examinations can help your gastroenterologists to confirm diverticular disease, including;
- A colonoscopy of your GI tract to look for possible diverticula at the entire length of your colon
- A CT scan to identify areas of inflammation and infected pouches
- A pregnancy test on women of childbearing age to rule out pregnancy as the cause of abdominal pain
The second part of your treatment would involve determining whether your condition is deemed complicated or not complicated.
Since about 25% of cases are complex, Australian guidelines now recommend outpatient treatment only for uncomplicated cases.
Outpatient management may involve antibiotic therapy, a liquid diet for specific days, a low-fibre diet until symptoms cease, and other pain relief medications. However, it is your doctor who will decide on the best treatment according to individual needs.
In case your condition is deemed complicated, it may require immediate intervention. Treatments for complex issues may include;
- Antibiotic therapies
- Intravenous fluids
- Medications to relieve symptoms
- A minimally invasive laparoscopic procedure to manage inflammation
- Surgery, in case your doctors need to remove bowel abscess, obstruction, or fistula from the colon and treat perforations
BetterHealth, (2012). Diverticulosis and diverticulitis. More information here.
Coble, J.(2017). Identification of a Rare LAMB4 Variant Associated with Familial Diverticulitis through Exome Sequencing (Human Molecular Genetics). More information here.
Healthdirect Australia, (2018). Diverticular Disease – Diverticulitis and Diverticulosis. More information here.
Marinella, M and Muhanad, M. (2000). Acute Diverticulitis in Patients 40 Years of Age and Younger. More information here.
Medical News Today, (2018) Everything you need to know about diverticulitis. More information here.
NHS Inform. (2020) Diverticular disease and diverticulitis. More information here.
Onur, et al. (2016). Diverticulitis: A Comprehensive Review with Usual and Unusual Complications. More information here.
Thompson, G. (2009) Diverticulosis and Diverticulitis – IFFGD. More information here.